

While we’ve only recently begun to talk openly about mental health and its importance in overall well-being, Mental Health Awareness Month has been observed in the U.S. since 1949 and is dedicated to education, addressing stigma, and advocating for policies that support the millions of Americans who experience mental health challenges. This year, the National Alliance on Mental Illness (NAMI) is celebrating with the More Than Enough campaign and invites us all to join via social media by tagging @NAMICommunicate and using the hashtag #MoreThanEnough and sharing a thought about how we are More Than Enough, regardless, despite, and adjacent to any mental health challenges we might be experiencing. In addition, SAMHSA is providing access to a toolkit for organizations to use to promote their own awareness campaigns.
As we think of Mental Health in general, we know that disorders rarely exist alone. Instead, individuals are more likely to experience a combination of challenges, often with overlapping symptoms. According to SAMHSA’s 2021 National Survey on Drug Use and Health, approximately 9.2 million adults in the U.S. experience co-occurring, or comorbid, mental health and substance use disorders. That number has increased from 7.7 million in data published by the National Institute on Drug Abuse (NIDA) in 2018.
Co-occurrence, or comorbidity is defined as having an experience of two or more mental health and substance use disorders either simultaneously or with one closely following the other. Of the 20.3M adults with substance use disorders in 2018, 37.9% also had mental health challenges and, of the 42.1M adults with mental health challenges, 18.2% also had substance use disorders. The interaction can create additional challenges for the course of treatment for both. Individuals with substance use disorders are at particular risk for developing one or more chronic diseases or chronic conditions.
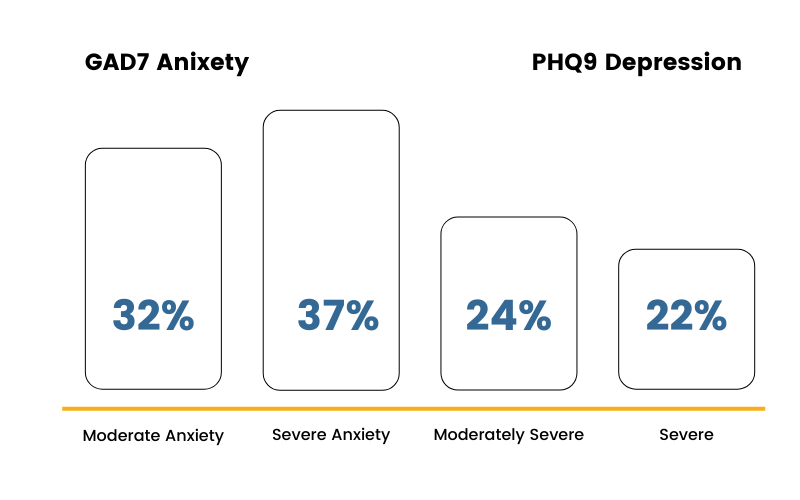
Looking specifically at a sample of over 5,000 individuals in substance use treatment across the care continuum using the ERP Health platform, approximately 45% report moderately severe or severe symptoms of depression and 68% of that same population report moderate or severe anxiety.
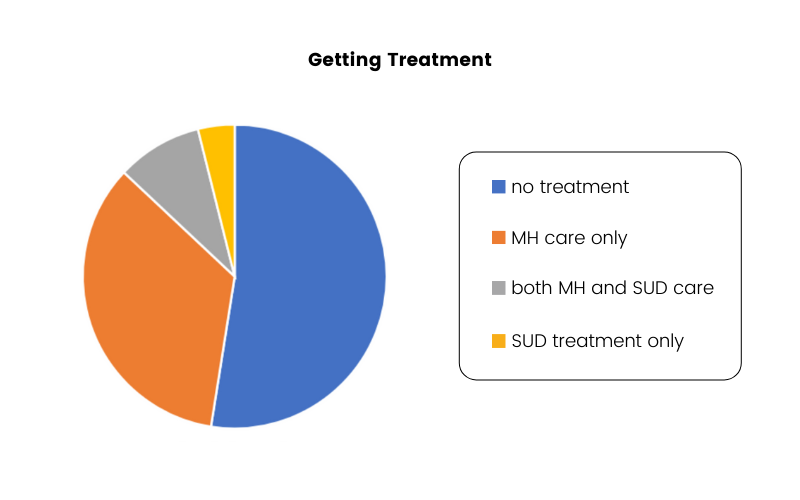
While it might be difficult to determine which came first (is primary), the symptom presentation will be different for every individual and the course of treatment will be determined by that individual’s needs. There are effective treatment approaches for both mental health and substance use disorders, however, an integrated approach to care will be the most effective for those with co-occurring problems. Unfortunately, not everyone who needs it gets a more comprehensive approach to care. According to data reported by NIDA, 52.5% received neither mental health care nor substance use treatment, 34.5% received mental health care only, 9.1% received mental health AND substance use, and 3.9% received substance use treatment only.
Barriers to Care
In many cases, even those who want to and are ready to seek care experience barriers to starting treatment. Over half (52%) of those with co-occurring disorders who did not receive mental health care described the main barrier as inability to afford care while approximately 24% of that population wasn’t sure where to go to get help and 23% thought they could handle the problem without treatment. On the other hand, of those with co-occurring disorders who did not receive substance use care, the main barriers to care were not being ready to stop using (38%), lack of health insurance and inability to afford care (35%), and concern for stigma-related impact on social relationships or job (13% each). According to Padwa et.al. (2015), there are additional systemic barriers, including organizational failure to sustain integrated care, limited support for co-occurring disorder treatment training, and diagnostic and billing restrictions.
Getting Connected to Care
Routine screening at multiple points of entry into healthcare can help address stigma, improve understanding of the connection between substance use and mental health challenges (health literacy), and provide the necessary nudges required to increase the likelihood someone will get connected to care. If an individual receives a behavioral health screening during an annual wellness or sick visit with their primary care provider, when in the emergency department or at urgent care, while visiting a community health center or pharmacy clinic, and even as a part of their workplace wellness program, they are more likely to be identified early and to receive care quicker than without routine screening and waiting until symptoms are unmanageable. Keeping mental health and substance use at the forefront of the total health discussion is essential to making any progress in co-occurring disorders.



